Standardizing how I measure and compare pain thresholds across different patients plays a huge part in both research and daily clinical care. Every person experiences pain in their own way, so clear and reliable methods help me spot real differences rather than just random variation or bias. By sticking with defined protocols, I can better compare outcomes, help identify effective treatments, and confidently discuss results with other clinicians or researchers.
Why Standardization in Pain Threshold Testing Matters
Pain thresholds tell me how much stimulus a person needs to report pain. These differences are not just about toughing it out; factors like genetics, medical history, mood, and environment all add up. When I use different methods, tools, or instructions, I can get very different results, even in the same person. That’s why having set steps is really important when my goal is to compare pain sensitivity between patients or groups.
For example, clinical research on chronic pain often relies on pain threshold data to track progress or test treatments. If everyone collects data differently, the results won’t line up, making it harder to learn what works. Standard protocols also make sure the process is fair for all patients and support accurate recordkeeping; both are super important in healthcare.
Using agreed-upon methods also strengthens my research if I want it published in peer-reviewed journals, where reviewers expect details on pain testing procedures. The more consistent my approach, the stronger my findings and recommendations become.
Expanding on this, following standardized pain threshold measurement is not only about making comparisons easier; it also helps track the effectiveness of interventions accurately. When I track pain thresholds over time and repeat the tests under the same conditions, I can see if a treatment truly gives a boost or if observed changes are just random.

Basics of Pain Threshold Measurement
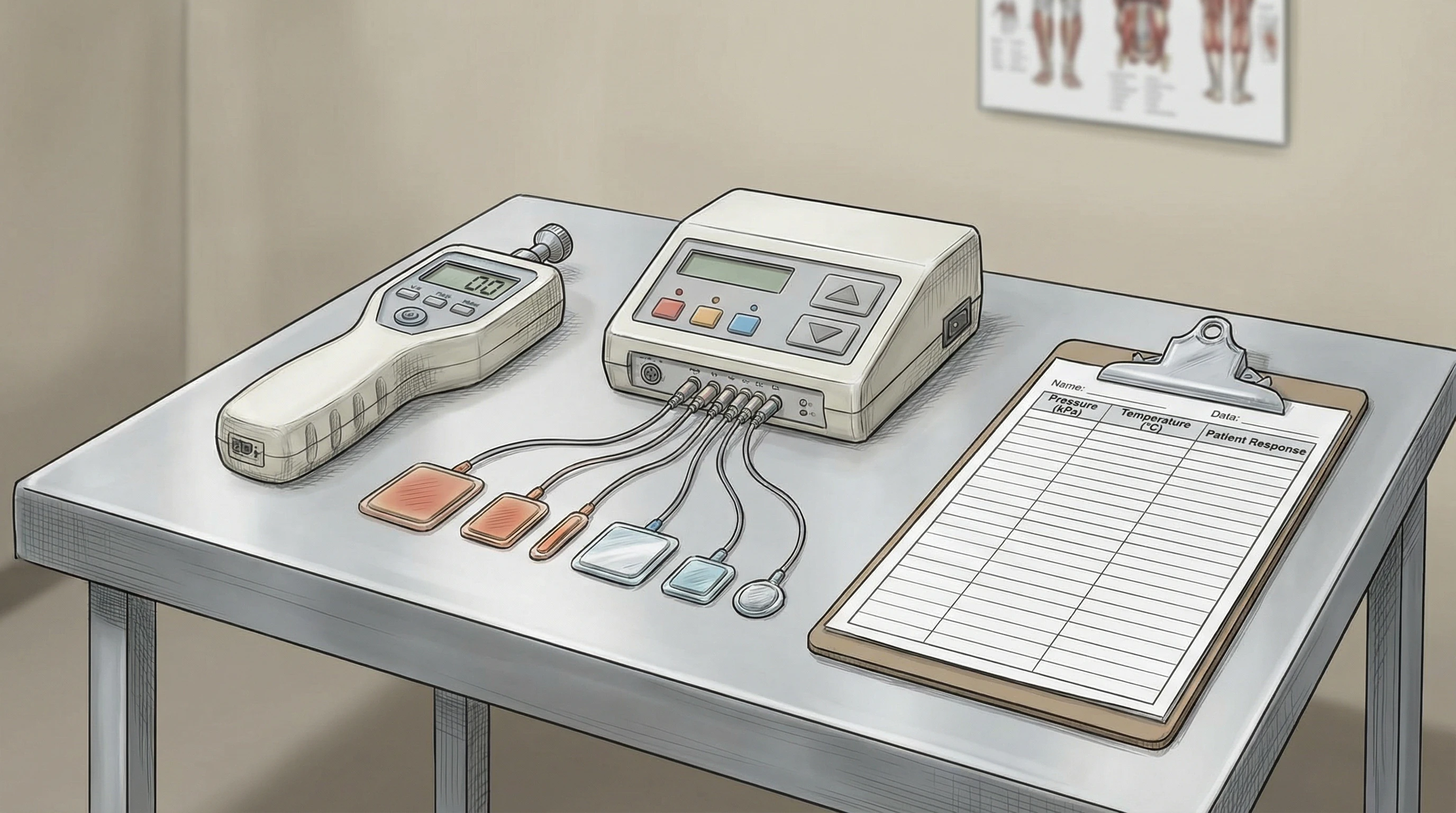
When I talk about pain thresholds, I’m usually interested in how much of a physical, thermal, electrical, or chemical stimulus it takes before someone first feels pain. I can use different types of tools or tests to do this, such as:
- Pressure Algometry: I press gradually on a muscle or joint using a device, noting the moment the person says it becomes painful.
- Thermal Testing: A small pad or probe heats or cools the skin, recording the temperature where the first pain sensation appears.
- Electrical Stimulation: Mild electrical pulses are delivered to the skin, with the patient alerting me when pain occurs.
- Chemical Methods: Sometimes, substances like capsaicin are used to trigger pain in a controlled way, mainly in research.
Tests like these help me compare results between people or before and after treatment. However, each method comes with its own learning curve and possible sources of error. That’s why sticking with clear instructions and reliable equipment is key.
Keeping protocols simple and repeatable ensures that even if there’s some difference in individual pain perception, the process itself remains steady. This consistency helps make sure the results are transferable between different clinics, researchers, or settings.
Core Elements of Standardized Protocols
For comparison across patients to really mean something, I make sure every step in my testing protocol is well-defined. Here’s what I focus on:
- Clear Instructions to Patients: I always explain what will happen and what I want them to do. For example, I might say, “Tell me the moment you feel the sensation turn into pain.” Consistent wording reduces confusion or hesitation.
- Calibration and Maintenance of Equipment: My devices (such as algometers and thermal stimulators) get checked before and after testing so I know results are accurate and repeatable.
- Standardized Stimulus Application: All trials use the same increase rate (like how quickly I press) or temperature change for every patient and session.
- Proper Environment: Keeping rooms at the same temperature, reducing noise, and following the same setup makes sure outside factors don’t skew results.
- Training and Familiarization: If I’m not used to the testing tools, extra practice and periodic refresher training help keep my testing smooth and reliable. Some studies suggest including a brief trial run so patients can get used to the process without feeling anxious.
By taking these steps, I control for the biggest sources of bias or error, which helps me trust that the differences I see are real and not just noise.
Documenting these standardized steps in clinical and research settings helps create a resource for others to follow and builds a foundation for future improvements. Protocols often develop further as new tools or techniques get introduced, so recording everything accurately is key for consistency over time.
How Standardization Helps Research and Practice
In clinical trials, using one agreed-upon protocol means I can combine data from many sites or compare groups based on location, condition, or treatment. Clear rules also cut down on disputes if results differ. For example, the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) offers consensus guidelines that many research teams use so their data can be easily compared or pooled (source: NIH).
In everyday clinical work, I may need to show that a patient’s pain response has changed after medication or therapy. Repeating the same protocol each visit ensures the improvement I see is genuine and not due to me changing the way I test. It also helps me spot patterns across groups, such as age or gender differences, giving me a general road map for further assessment or targeted support.
On top of that, having an all-in-one reference for protocols helps when teaching new staff or guiding trainees. Everyone benefits from seeing how standardized approaches improve reliability and patient care.
Challenges When Implementing Standardized Protocols
I have run into a few common roadblocks:
- Some patients have trouble understanding instructions, especially young children or those with language barriers.
- Not all clinics have the same equipment, or it might be older and less precise.
- Different conditions can affect pain reporting, like anxiety, fatigue, or cognitive changes.
- Staff might use slightly different phrasing out of habit, or have slightly varied testing techniques.
Even with protocols, complete uniformity is tough. Regular team training and clear written guides help. Translating patient instructions into multiple languages and considering cultural differences also play a part in improving understanding. For patients with communication challenges, some protocols use visual scales, like the Wong Baker FACES scale, or hand signals instead of verbal responses.
Advances in technology are making it easier to smooth the way for standardization by creating automated tools for pain measurement, or apps that help guide both providers and patients through each step. These tools offer built-in reminders for calibration and instructions, making it easier to maintain consistency.
The Importance of Consistency in Data Collection
If I want pain threshold results that actually reflect patient differences, I remind myself that consistency in data collection is as important as the tools themselves. Even something as simple as room temperature or how I phrase a question can change the outcome. Double-checking my steps and teaming up with colleagues helps keep things on track.
Documentation and Recordkeeping
Documenting exactly how the test was done, noting any variations, and recording conditions during the test help make my findings much more reliable. Many facilities keep digital templates that prompt clinicians to log the calibration status, environmental factors, and any patient hesitations or questions. This builds trust in the results for research, audit, or future care planning.
Regular audits of documentation and calibration records can also identify areas for improvement, allowing the clinic to adjust protocols when needed. Transparent and timely recordkeeping helps meeting standards for regulatory bodies and supports stronger clinical outcomes.
Using Pain Threshold Comparisons in Practice
There are many ways standardized pain threshold testing can be put to work:
- Chronic Pain Assessment: Tracking a patient’s pain threshold over time, especially before and after treatment.
- Evaluating New Treatments: Comparing changes in pain sensitivity with medicine, physical therapy, or devices.
- Group Studies: Looking for pain differences across ages, genders, or specific conditions like neuropathy versus arthritis.
- Screening for Rare Conditions: Some rare genetic disorders can show unique patterns of pain sensitivity.
Standardized methods help me feel confident that I’m actually seeing real changes, not just random swings or mistakes in test delivery.
Standardized pain threshold data can also be useful in legal settings. For example, workers’ compensation claims or insurance assessments may use such information to document injury severity or progress. Having reliable, repeatable methods gives extra confidence when providing expert opinions.
Frequently Asked Questions
Some questions often come up when discussing pain testing between patients or in research settings. I’ll share a few that I often hear:
Question: What’s the best method for measuring pain threshold?
Answer: There is no single best way, since each method (pressure, thermal, electrical, or chemical) suits different situations and patient needs. I choose the method based on the clinical or research question, type of pain, and available tools. Standardizing within the method I choose is what matters most.
Question: How can I reduce bias during pain threshold testing?
Answer: I use precise instructions, test in a stable environment, calibrate equipment before each session, and record any deviations from the normal protocol. If possible, I also blind the patient to details like target temperature or pressure, so they focus only on their experience.
Question: Is pain threshold testing uncomfortable or risky?
Answer: Pain threshold testing is designed to stop as soon as the first pain is felt, well before harm occurs. I always monitor patients closely and stop immediately at their request. Some people may feel anxiety about the test, so I explain everything clearly to put them at ease.
Question: Do factors like mood or fatigue affect test outcomes?
Answer: Yes; mood, anxiety, tiredness, and even recent medication use can impact a person’s response to pain stimuli. That’s why I try to test under similar conditions each time and document these factors, so any changes seen are more likely to be real differences rather than temporary influences.
My Experience with Pain Threshold Testing
I have found standardized pain threshold testing really useful when working with patients managing ongoing pain conditions. Explaining the process helps put people at ease, and sticking to the same method every time means I can trust small changes I notice. In a clinic setting, having written checklists makes it easier for new team members or visiting trainees to keep care consistent. If you’re interested in more technical resources or want to see guidelines, I suggest checking out the latest consensus statements from groups like IMMPACT or reviewing protocol papers on PubMed.
Picking a simple, repeatable method that fits the needs of both the clinic and patient makes the whole process smoother for everyone. This supports better care decisions in the long run and helps deliver the most accurate understanding of pain management progress.
Wrapping up, being dedicated to detailed, standardized testing protocols lets me give a boost to the quality of my care and research, making real improvements for both patients and the scientific community.